
Traiter l’obésité sévère sans véritable opération…
L’endo-plicature gastrique est-elle une révolution ?
Parmi les techniques « par les voies naturelles », l’endo-plicature est certainement celle qui attire le plus de commentaires et semble porteuse des meilleurs promesses.
Elle se traduit par un réel engouement parce qu’elle répond aux besoins du « monde bariatrique » et au-delà de la société dans son ensemble, à la recherche de meilleurs compromis, bref d’une meilleure acceptabilité, ce que nous traduisons en termes médicaux par un bon rapport bénéfice/risque.
D’autre part, et c’est la bonne nouvelle de l’été 2022, elle est validée par la plus haute autorité de santé en France (HAS) dans un cadre de recherche encore limité, du moins concernant sa prise en charge : patients avec diabète de type 2, dans un centre habilité, avec un IMC compris entre 30 et 35 kg/m2, et avec pour le moment le seul dispositif ENDOMINA (Endotools TherapeuticsTM).
Les atouts de l’endo-plicature
Apparue en 2007 sous l’impulsion d’un chirurgien vénézuélien (Fogel) cette technique repose sur un principe très simple : rétrécir la lumière de l’estomac par une action de pliure ou plicature, au moyen de fils par exemple noués sur la surface interne de l’estomac de diverses manières. On essaie ainsi de répliquer ce qui est réalisé de manière plus radicale lors de la sleeve gastrectomie, intervention qui enlève complètement les deux-tiers de l’estomac après que celui-ci ait été sectionné dans le sens de la hauteur.
Il existe bizarrement deux concept chirurgicaux qui reproduisent également cette façon de faire: l’un est expérimental et récent (le sleeve-gastroclip), l’autre déjà ancien de plus de 10 ans mais quasiment tombé en désuétude, la « sleeve-plicature », où l’estomac est non pas enlevé mais également plié, cette fois-ci de l’extérieur, transformant sa paroi en une sorte de saucisson !
Il faut bien comprendre le saut que cela représente, tout aussi important que celui qui a eu lieu il y a une quarantaine d’années, lorsque la coelioscopie (ou laparoscopie) a progressivement en en grande partie remplacé la voie d’abord traditionnelle consistant à « ouvrir le ventre » (laparotomie) ; le fait aujourd’hui d’avoir la possibilité, encore pas totalement aboutie bien sûr, de passer entièrement par les voies naturelles (l’œsophage et l’estomac) sans aucune cicatrice abdominale est assurément nettement plus attractif .
Comment cela marche-t-il ?
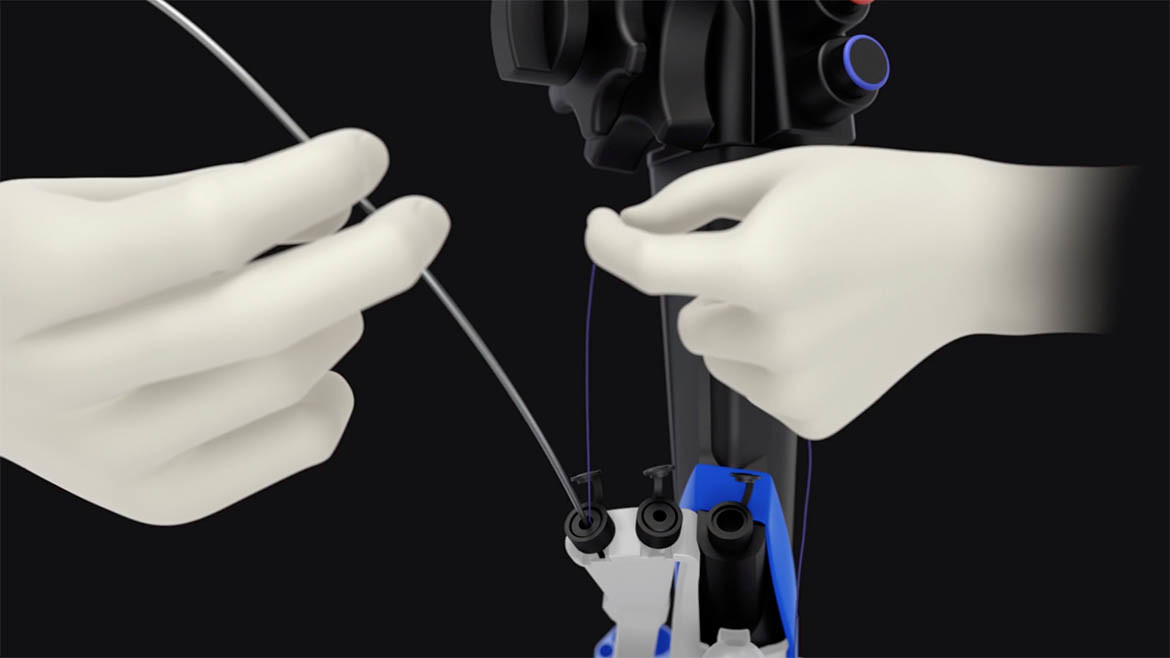
Comme son alter ego chirurgical, la plicature endoscopique repose sur le principe d’un rétrécissement de l’estomac, mais de l’intérieur, et grâce aux progrès du matériel de suture. Il ne faut pas oublier que le challenge a été de concevoir un dispositif de suture, assez banal en chirurgie classique, mais ici au bout d’un instrument de plus de 130 cm de long soit un endoscope qui sert quotidiennement pour explorer l’estomac.
Quels sont les risques?
Ils sont très faibles. Toutefois la mise en place de points et sutures profonds à partir de l’intérieur de l’estomac entraine deux risques, plutôt théoriques que réels et dans la pratique assez rarement décrits: l’hémorragie (qui peut requérir une nouvelle endoscopie pour la contrôler, voire une transfusion, ce qui est exceptionnel), et la perforation de l’estomac: à vrai dire, c’est assez fréquent mais minime car les aiguilles utilisées sont fines, et il n’est pas rare d’observer de l’air sur une radio de l’abdomen, alors que cela n’a pas de traduction en termes de symptômes sinon des douleurs modérées dans les épaules durant quelques jours.
Il est aujourd’hui rassurant de constater l’absence ou la grande rareté de complication sérieuse rapportée jusqu’à présent, alors que l’on pourrait anticiper des problèmes tels que ulcérations, saignements, perforation, etc. Ceux-ci ne peuvent être écartés, mais demeurent exceptionnels, en tous cas pas davantage que pour le ballon gastrique, donc très inférieurs à ceux d’une chirurgie classique.
Comment s’alimenter ensuite ?
De manière semi-liquide, fractionnée et moulinée pendant quelques jours, sans contrainte ni restriction particulière, en évitant de boire et manger en même temps. Puis assez rapidement de manière normale en petites quantités, avec 2-3 semaines de prudence.
Quels sont les résultats ?
Il semble que les résultats soient meilleurs que ceux du ballon gastrique en terme de perte de poids: plutôt 20% que 15% de perte de poids total; et surtout plus durables, au delà de 1 an, et sans doute 18-24 mois. Il est trop tôt pour se prononcer, car il n’existe qu’un nombre insuffisant de centres expérimentés (Espagne, USA, Arabie Saoudite), mais déjà des séries de patients importantes et avec un recul de 5 ans pour les plus anciennes.
Un argument mis en avant par les promoteurs de cette méthode est celui de son caractère « répétable à la demande », mais là encore il est prématuré d’en faire une stratégie de routine.
* Articles récents concernant les trois principales techniques :
– Endomina: Huberty V et al, 2020, Gut. Endoscopic sutured gastroplasty in addition to lifestyle modifications (Gastroplastie endoscopique en complément de modifications diététiques). Efficacité à court terme lors d’un essai contrôlé et randomisé. Deux patients sur trois bénéficiaient de la technique Endomina (71 patients), et 1/3 du traitement conventionnel: la perte de poids a été 25% meilleure à 6 mois dans le groupe traité. A 6 mois, la perte de poids a été de 38,6% dans le groupe traité contre 13,4% dans le groupe contrôle; à 12 mois 45,1% contre 11,8%. De même, de meilleurs résultats ont été obtenus en termes de tests de qualité de vie, et de tests de satiété.
– Apollo: Pizzicannella et al, 2020, Surgical Endoscopy. Does endoscopic sleeve gastroplasty stand the test of time? Objective assessment of endoscopic ESG appearance and its relation to weight loss in a large group of patients (Est-ce que la sleeve gastroplastie endoscopique passe le test du temps? Evaluation objective de l’ESG et de sa relation à la perte de poids dans un large groupe de patients). Trois aspects différents de la sleeve ont été évalués lors d’une endoscopie de contrôle à 6 et 12 mois post-opératoires: plicature ouverte (c’est-à-dire théoriquement inefficace), plicature partiellement intacte ou intacte, chez 133 ESG réalisée d’ octobre 2016 à avril 2017. 7% des patients avaient une plicature ouverte, 44% une plicature partiellement intacte et 49% une plicature intacte. 41 patients étaient disponibles pour une évaluation à 12 mois. La perte d’excès de poids était de 34,8% +/- 22 à 12 mois, et les chiffres étaient bien corrélés avec le statut de la plicature.
– USGI (POSE): Abu Dayyeh et al, 2021. Greater gastric curvature endoscopic tubularization using snowshoe anchors for weight loss: a first inhuman pilot prospective feasibility study of the Pose 2.0 procedure (Tubulisation endoscopique de la grande courbure gastrique avec des ancres-raquettes pour perte de poids; une première étude chez l’homme de la technique Pose 2.0). 13 patients ont été opérés de août à novembre 2017; la durée moyenne d’intervention a été de 36+/-11 min, 18 plicatures séparées ont été réalisées; il n’y a eu aucun effet indésirable grave; la perte de poids a été de 11,5% et la perte d’excès de poids (EWL) de 36%.
Coûts
Le coût tout compris d’une endo-plicature à PLN (Polyclinique Lyon Nord) est de 6 000 €. Ceci comporte le matériel principalement (environ 4 000 €), et les honoraires de l’équipe multi-disciplinaire, incluant le suivi pendant 6 mois.
Démarches pratiques en vue et durant le séjour pour une endo-plicature
– La consultation pré-opératoire: elle est indispensable pour d’une part recueillir tous les éléments de votre état de santé, votre index de masse corporelle ou IMC (poids/taille au m2) et d’autre part vous informer complètement.
– La préparation à l’intervention fait appel à d’autres professionnels de santé, comme la diététicienne, l’éducateur physique, etc.
– L’intervention elle-même: pourrait être faite en ambulatoire, néanmoins comme il s’agit d’une technique nouvelle et « hors sécurité sociale » (sauf par dérogation dans le cadre de l’étude validée par la HAS et débutant en France), nous préférons par sécurité garder les patients une nuit, d’autant que la plupart sont domiciliés assez loin de l’établissement. L’entrée se fait le plus souvent le matin même de l’intervention.
La durée est de 1 heure environ. Le patient reste en salle de réveil en général 1 heure également, puis dès son retour a la possibilité de prendre un peu de liquide, et se lever.
– Le traitement post-opératoire: il comporte trois éléments, un médicament pour les nausées et éventuels vomissements, un pour les douleurs (parfois à forme de spasmes), enfin le plus important car il doit être poursuivi au-delà des quelques jours après l’intervention, un médicament anti-acide (que l’on appelle IPP, la molécule générique de référence étant l’oméprazole). L’alimentation est dès lors reprise normalement, en petites quantités, de manière semi-liquide (consistance de « pots-bébés ») ou moulinée (purées, viande hachée, etc.); l’aide de l’équipe multi-disciplinaire s’avère alors très utile.
Liens internet
Le site plus abouti est celui de la société APOLLO : www.apollosurgical.com
Sélectionnez : Home | OverStitch™ Endoscopic Suturing System
Beaucoup de détails, un site bien à jour et regroupant les autres technologies de cette société, notamment le ballon gastrique.
Site sobre, avec quelques informations, le Société ne vend pas directement en France directement à ce jour.
Peu d’information (mais nette amélioration récemment) ce qui est dommage, mais un schéma du dispositif et des vidéos.
Treating obesity without a real operation: Gastric Endo-Plication (Gastric Endo-Sleeve), a revolution?
Obesity never stops growing, not only in France (as shown in the latest data from the OBEPI inquiry), but also in the rest of the world, affecting more than 800 million people across the globe. Conventional treatments, mostly represented by diet and lifestyle intervention, are most of the time insufficient or inefficacious, even frustrating eventually: many patients are relying on poorly tested methods, with very short-term effects, at times dangerous, and experience deleterious weight-cycling. Bariatric surgery concerns only a small proportion of patients, the very obese ones (Body Mass Index or BMI> 40 kg/square meter), and this surgically treated fraction diminishes while obesity prevalence increases, because it mobilizes important resources that are finally excessive in the current environment context and given other health priorities…
Why dedicating a large part of an informative website to an operation that is not supposed to be enough mature and/or insufficiently tested?
Because it is attractive and very efficient? No, that would not be enough! The true reason is the change in mindset regarding medical technologies: it evolves and concerns society as a whole, alongside the quest for better compromises, which in medical terms we translate into « a reasonable benefit/risk ratio ». In the same time, there is obviously around the world a momentum towards less aggressive techniques than laparoscopic surgery because of complications and/or long-term uncertainties; preserving the environment and diminishing the greenhouse gas emissions is another trend, various publications having alerted about the global input of the health industry in general (7% of global emissions), with a dominant part from the surgical suites, up to half of the emissions of a given hospital.
Let us make a daring comparison: in 2035, the European Union will begin to phase out cars using fossil gas fuel (in other words electric vehicles will become dominant). We may imagine that the same evolution could take place regarding the respective parts of bariatric surgery and bariatric endoscopy! Stronger investments into endoscopic technologies would be required, but they are unlikely for the time beeing since major companies take advantage of the current thriving market of the procedures that entail stapling of the stomach.
Let us take the compelling example of the most common bariatric procedure, sleeve gastrectomy. Up to 1.5 kg single-use material is « wasted » for each procedure (i.e. stapling, reloads, energy device for sealing vessels and dividing adhesions, etc.), and up to 3 kg of other waste. Two-thirds are represented by plastic material, versus one third of metallic waste, everything being incinerated at 850°C, most of the time without any recycling process. The remaining waste accounts for some 1,5kg. It has been calculated that on average, a surgical intervention was responsible for roughly a 120 kg CO2 output, i.e. the weekly energy expenses of a four-person family.
– Surgery: 1) A model that has become rapidly universal, sleeve gastrectomy, 2) For the time being, other types of interventions are almost always derived from gastric bypass, either the most classical one (called Roux-en-Y gastric bypass), or numerous variations. These models encounter difficulties nowadays. Bypass remains rather unpopular because of its complexity, potential complications and the lifelong necessity of supplements (micro and macro-nutrients and vitamins) and surveillance. Regarding sleeve, one has deemed for a long period of time that the main pitfall was the occurrence of postoperative complications, i.e. bleeding, leak or stenosis, leak being dread because somehow difficult to treat although rarer (1-3%). In the longer term however, the number one issue has become gastro-esophageal acid reflux, because the gastroesophageal junction becomes virtually incompetent, necessitating regular surveillance through upper GI endoscopy starting on year 3 postoperatively and for an indefinite time.
– Endoscopy: Traditionally, digestive endoscopy has mostly an exploratory purpose, meaning that for obese patients it is instrumental in evaluating the status of the digestive tract (esophagus and stomach lumen). More recently, it has also been proven useful for treating some complications, for example leaks (plugging), ulcers, stenosis (stents), and bleeding. Becoming more ambitious, upper GI endoscopy may treat primary cases of obesity. Theoretically, and in accordance with most scientific societies albeit with nuances (surgeons and endoscopists do not always share the same point of view), patients that are referred to endoscopists are preferably those who are not eligible for surgery, or contra-indicated for surgery (fragile patients, older patients…), and/or who are just overweight but with really morbid conditions, for example with a Body Mass Index (BMI) below 35 kg/m2 and a type 2 diabetes, or finally not willing to undergo surgery.
There are: 1) An old benchmark, the Intra Gastric Balloon, 2) Various medical devices on display, most of the time under research protocols with no formal success and/or acknowledgement, 3) The endo-plication, so far the most promising with the perspective to become established as an independent and worthwhile weight-loss procedure.
1) For more than 40 years, the benchmark intervention has been the Intra Gastric Balloon. This is solid ground, with thousands of research papers, hundreds of thousands of devices sold around the world and diverse brands, from the typical 6 month-ORBERA balloon to longer duration balloons (up to 12 months or even more, which is not necessarily more efficient), balloons that can be refilled (which necessitates an additional anesthesia); last but not least (although skipping endoscopy), a new balloon that can be swallowed has been commercialized with some success for 8 years, because neither anesthesia nor endoscopy are necessary.
2) Interventions at the research stage: they are numerous and varied, with a recent momentum in favor of the so called « metabolic procedures ». In order to understand this concept, you have to refer to surgery. Modern trends in surgery insist more than ever on the so called « metabolic syndrome », namely the association of elevated blood pressure and blood sugar as well as lipids (cholesterol) and triglycerides, and less on weight-loss per se. In this respect, one usually recommends interventions that aim at this improvement, rather than solely weight loss with restriction of food intake. The idea of metabolic techniques encompasses what we call malabsorption that mostly deals with bypass procedures, that has a large variety of spin-offs.
Given this success, one may ask if this idea can be also applied to endoscopic techniques. Several trials are going on, let us cite the three main projects that aim at type 2 diabetes improvement rather than weight-loss solely:
– The « Sleeve Endobarrier »: a complicated word for a simple idea, that consists in inserting a plastic tube at the bottom of the stomach (the duodenum), which is then deployed inside the initial bowel segments (the jejunum), impeding a perfect admixture of food and bilio-pancreatic secretions. This makes it more or less similar to the effect of the surgical gastric bypass.
– The so-called « Duodenal Rejuvinating » (FRACTYL): a daring procedure that has a similar background, i.e. altering the duodenal mucosa through what is called thermo-abrasion, i.e. a mild and superficial burning.
– The partial jejuno-ileal bypass (which entails a suturing-anastomosis) connects two portions of the small intestine, thereby short-circuiting a large part of it, through endoscopic magnets. This mimics an old and highly debated operation, the ileo-jejunal bypass, but supposedly without its deleterious effects. One may act likewise for anastomosing the stomach and the jejunum, but this is currently much more experimental.
3) Why is gastric endo-plication an asset?
This initial publication regarding this technique dates back to 2007 by a Venezuelan surgeon (Fogel), and rests upon a simple principle: narrowing the intra-gastric lumen through plication, with stitches or any other means (staples have been tested as well). This is more or less a replicant of the « real » sleeve gastrectomy, which takes off two-thirds of the stomach after being divided from bottom to top.
Oddly enough, there are two surgical concepts that apply to this: the first one is still experimental and recent, the so-called sleeve Gastro-clip, the second one dates back 10 years from now and has decayed ever since: the « sleeve-plication » entails an external running suture (with one or two layers), transforming the stomach into a kind of sausage!
How does it work?
Like its surgical counter-part, the ESG (for Endoscopic Sleeve Gastroplasty) narrows the gastric lumen, but from the inside, and through suturing material (not staples). One has to remember that the challenge has been to transform a rather mundane surgical suturing device into one that could be manipulated from a 130 cm distance, at the tip of an endoscope that goes deep into the gastric lumen!
What are the risks?
They are quite low. Yet placing stitches deep inside the gastric wall entails two risks, that are practically more theoretical than real (less than 2% severe adverse events): bleeding may require a new endoscopy to clean the hemorrhage and control the vessels that may bleed; perforation may occur, it is often very mild (thanks to the tiny size of the needles that are being used): one sees air on a radio of the abdomen and patients experience moderate pain in the shoulders for a few days. It is nowadays reassuring to observe that very few serious complications have been reported so far, as it is the case with gastric balloons, and of course to a much lower extent than the complications that occur after bariatric surgery.
How does one take food after the procedure?
It has to be semi-liquid, fractioned and mashed for a few days, without particular restrictions, avoiding to eat and drink at the same time. Normal food with small amounts is then recommended.
What are the results?
They seem to be better than those of the gastric balloon: 20% Total Body Weight Loss Vs 10-15% with the balloon; they are also more durable, beyond 1 year and even 18 months. It is too early to be assertive concerning results beyond 2 years, because only few centers have gathered a large experience (Spain, USA, Saudi-Arabia…), and/or have published sound data. Promotors put forward a strong argument: the method can be reproduced « on demand », but it is premature to establish it as a routine strategy.
*Recent publications are available concerning the three most important devices:
– Endomina: Huberty V et al, 2020, Gut. Endoscopic sutured gastroplasty in addition to lifestyle modifications. Short-term efficacy in a controlled randomized trial. 2/1 LSI (Life style Intervention) Vs LSI + Endomina in 71 patients: Weight-loss was 25% better WL at 6 months in the treated group. At 6 months 38.6% EWL in treated group Vs 13.4 in control. At 12 months 45.1% EWL Vs 11.8%. Likewise, better results were obtained in terms of QOL tests (Quality of Life) and satiety tests.
– Apollo: Pizzicannella et al, 2020, Surgical Endoscopy. Does endoscopic sleeve gastroplasty stand the test of time? Objective assessment of endoscopic ESG appearance and its relation to weight loss in a large group of patients. Three aspects were evaluated during an endoscopy at 6-12 months post-operatively: open plication, partially intact or intact, in 133 ESG between Oct 2016 and April 2017. There were 7>% of patients with an open plication, 44% with a partially intact plication and 49% with an intact plication. 41 patients were available at 12 months for evaluation. EWL% was 34.8 +/- 22 at 12 months, and the numbers correlated with the suturing status.
– USGI (POSE): Abu Dayyeh et al, 2021. Greater gastric curvature endoscopic tubularization using snowshoe anchors for weight loss: a first inhuman pilot prospective feasibility study of the Pose 2.0 procedure. 13 patients were operated on from August to November 2017; average duration was 36+/-11 min, 18 plications were carried out; no SAE (Severe Adverse Event) were reported, average weight loss was 11.5% WL and Excess-Weight loss 36%.
Costs
The cost for an endoplication at the PLN (Polyclinique Lyon Nord), all inclusive, is 7300 €. This includes the device (around 4000€), the fees for the hospital, and the fees for the multi-disciplinary team, with a 6 months follow-up.
Road-map to the operation and hospital stay
– Preoperative visit and counselling.
– The procedure itself: it may be done in an ambulatory setting (outpatient), although we prefer to keep most patients for one night if they live far away from the hospital. Entrance takes place the very morning of the procedure. The duration of the intervention is usually less than an hour, + one hour in the recovery room. Then the patient may ambulate and have some liquids to drink.
– Postoperative cares include an anti-acid drug (called PPI, for example omeprazole). Food intake can be almost normal, small amounts at a time, semi-liquid in the first place. The assistance of our multi-disciplinary team may be requested.
Internet links
Select : Home | OverStitch™ Endoscopic Suturing System
A lot of details, well made website with other information on Apollo devices (such as balloons)
A few information, but this company does not sell much in Europe
Very few information unfortunately